This is an online Elog book to discuss our patient deidentified health data shared after taking his/ her guardians sign informed consent
Here we discuss our individual patient problems through series of inputs from available Global online community of experts with n aim to solve those patient clinical problem with collect current best evidence based input
This Elog also reflects my patient centered online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of " Patient clinical data analysis" to develop my competancy in reading and comprehending clinical data including history, clinical finding, investigations and come up with a diagnosis and treatment plan
CONSENT AND DEIDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed through out the piece of work whomsoever

On June 2022 went to vemulokonda hospital got tt and vaccinated for monkey scratch
Not a known case of DM/CAD/EPILEPSY/TB/ASTHMA
PERSONAL HISTORY
married at age of 18, has two daughters
No smoking and alcohol history
Bowel and bladder: regular
Diet: mixed non vegetarian
Sleep: adequate
Appetite: normal
No known allergies
FAMILY HISTORY
Father died of TB 35 years ago
Mother has osteoarthritis and HTN since 1 year
No family history of Diabetes, CAD, Cancer, psychiatric illness, epilepsy
GENERAL EXAMINATION:
PATIENT IS CONSCIOUS ,COHERENT AND COOPERATIVE.
ORIENTED TO PLACE, PERSON BUT NOT TIME
NO PALOR ,ICTERUS, CYANOSIS, LYMPHADENOPATHY, EDEMA
VITALS AT ADMISSION:
BP: 110/80MMHG
PR: 88BPM
RR: 18CPM
SPO2: 98%AT RA
TEMP 98°F
SYSTEMIC EXAMINATION:
CVS: S1,S2 HEARD
RS: BAE+
CNS:
HIGHER MOTOR FUNCTIONS:
Consciousness - conscious
Oriented time x place ✓ person ✓
Speech and language - n
Memory
- immediate - retention decreased
Recall decreased
recent decreased
remote ✓
Delusions and hallucinations absent
MMSE SCORE 25/30
CRANIAL NERVES RIGHT LEFT
CN 1 Normal
CN 2. Field of vision ⬇️. ⬇️
Colour vision. N. N
CN 3 4 6 Extra ocular movements. N. ⬇️
Pupil size NSRL. NSRL
Direct, Indirect reflex N. N.
Accomodation. N. N
Ptosis absent. Absent
Nystagmus. absent. Present
CN 5. Sensory and motor reflexes normal
Jaw jerk Absent
CN 7 ,8 ,9,10,11,12. Normal on both sides
MOTOR: TONE NORMAL, POWER IN BOTH UL IS 5/5, IN BOTH LL IS 4+/5
CEREBELLAR SIGNS:
ATAXIA - SWAYING TO LEFT
NYSTAGMUS PRESENT IN LEFT EYE TO THE LEFT
NO DYSARTHRIA
NO HYPOTONIA
TITUBATION ABSENT
NO INTENTION TREMOR
PENDULAR KNEE JERK ABSENT
UL CORORDINATION
FINGER NOSE TEST POSITIVE
FINGER FINGER TEST POSITIVE
(NO COORDINATION )
LL. HEEL KNEE TEST
Rt. Lt
++. -
RT. LT
DYSDIADOKINESIA +. +
MOTOR: TONE NORMAL, POWER IN BOTH UL IS 5/5, IN BOTH LL IS 4+/5
REFLEXES ON BOTH SIDES:
B ++
T ++
S +
K +
A +
P F
P/A: SOFT, NON TENDER
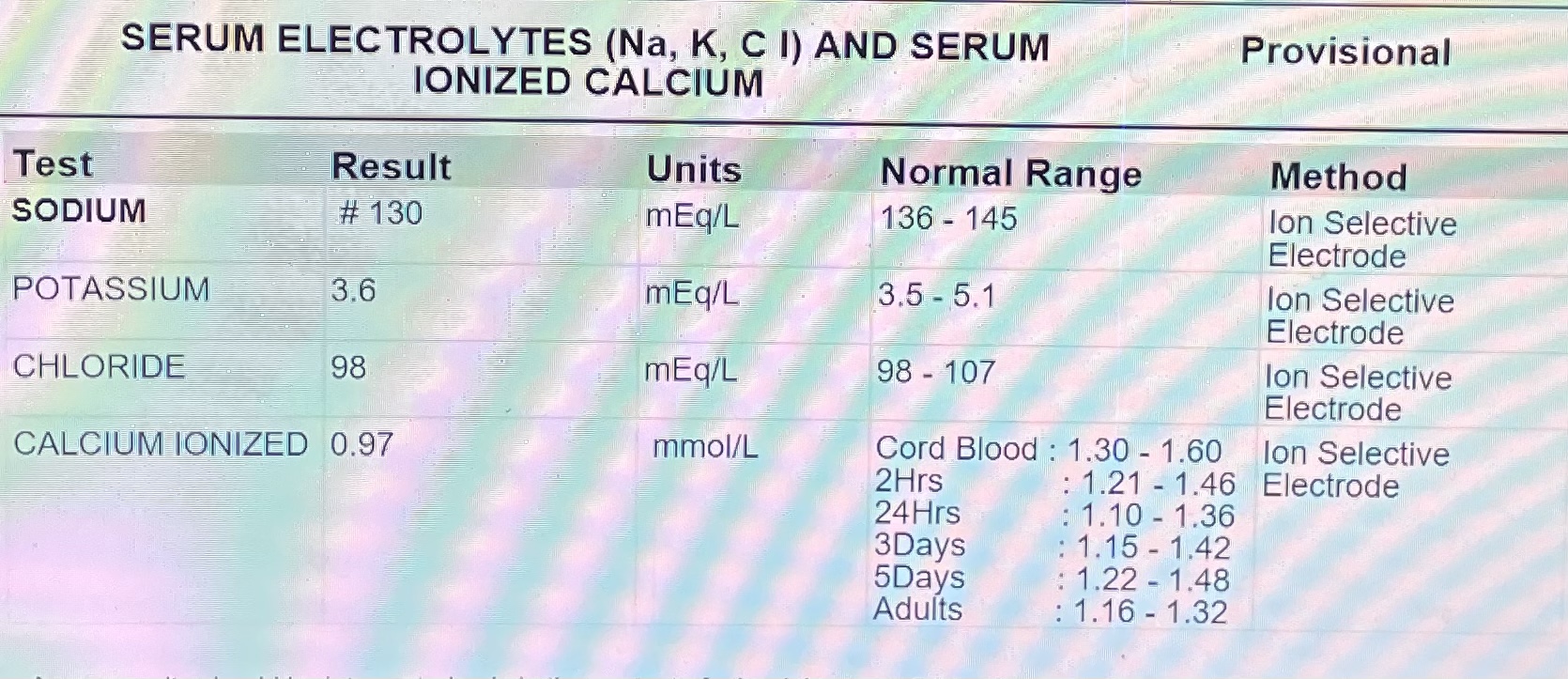
OUTSIDE INVESTIGATIONS























Day 2 AMC




Day 3




44x41x42mm Peripherally enhancing thick irregular wall intra axial lesion in left cerebellar hemisphere extending into vermis
Lesion is causing compression and displacement of 4rth ventricle to contralateral side with resultant mild dilatation of lateral and 3rd ventricle suggestive of acute hydrocephalus
Periventricular hyperintensity suggestive of transependymal sepage of CSF
PROVISIONAL DIAGNOSIS:
1.Chronic vomitings since 2 months secondary to ?lt Cerebellar lesion compressing 4th ventricle ? Acute hydrocephalus secondary Mets? Primary brain malignancy
2.k/c/o htn since 2 yrs with b/l OA knee grade 4, lt more than rt
Day 1 treatment
INJ ZOFER 4MG IV TID
INJ PAN 80MG IN 50ML NS CONT IV INFUSION
IVF AT 75ML/HR
ORS 1 PACKET IN GLASS OF WATER IN SIPS
GRBS 4TH HRLY
Day 2 treatment
INJ OPTINEURON 1AMP +100 ML NS IV OD
INJ ZOFER 4MG IV TID
TAB PAN D 40/30 PO/BD
IVF AT 75ML/HR
ORS 1 PACKET IN GLASS OF WATER IN SIPS
PROCTOLYTIC ENEMA
Day 3 treatment
INJ OPTINEURON 1AMP +100 ML NS IV OD
INJ ZOFER 4MG IV TID
TAB PAN D 40/30 PO/BD
IVF AT 75ML/HR
ORS 1 PACKET IN GLASS OF WATER IN SIPS
TAB AMLONG 5MG PO OD
Day 4 treatment
INJ OPTINEURON 1AMP +100 ML NS IV OD
INJ ZOFER 4MG IV TID
TAB PAN D 40/30 PO/BD
IVF AT 30ML/HR
TAB SHELCAL CT PO OD
TAB JOINTACE PO OD
D2 INJ LEVERA 500MG IV BD
D2 INJ DEXA 8MG IV TID
Comments
Post a Comment